Real-time feedback loops in HCC coding can help clinicians correct mistakes instantly and learn from them. Traditional methods of improving coding accuracy often rely on retrospective audits, which may take weeks or months before clinicians receive insights. This delay can result in missed opportunities for accurate documentation and increased administrative burden.
By integrating real-time feedback, clinicians can receive immediate guidance, make corrections on the spot, and reinforce best practices. More importantly, it fosters a culture of continuous improvement, reducing repetitive errors and ensuring compliance with evolving coding guidelines.
Healthcare organizations can proactively support clinicians rather than rely solely on post-service audits, enabling more efficient workflows and better patient care.
That’s why this article will explore the steps, challenges, and best practices for setting up real-time feedback loops in HCC coding, ensuring they are constructive, efficient, and lead to measurable improvements.
Understanding Real-Time Feedback Loops in HCC Coding
To implement this kind of system, organizations must first establish key components:
-
- Data Collection & Identification of Gaps
- Review & Analysis of the Data
- Feedback Delivery to Clinicians
- Justification & Training for Improvement
Each step is critical in creating a seamless loop where clinicians receive feedback on documentation errors or omissions and adjust their practices accordingly. Whether from software, trained personnel, or a hybrid approach, you must ensure the system functions efficiently.
Step 1: Data Collection & Identifying Gaps
The foundation of real-time feedback lies in identifying where clinicians struggle. Your organization can do this in several ways:
-
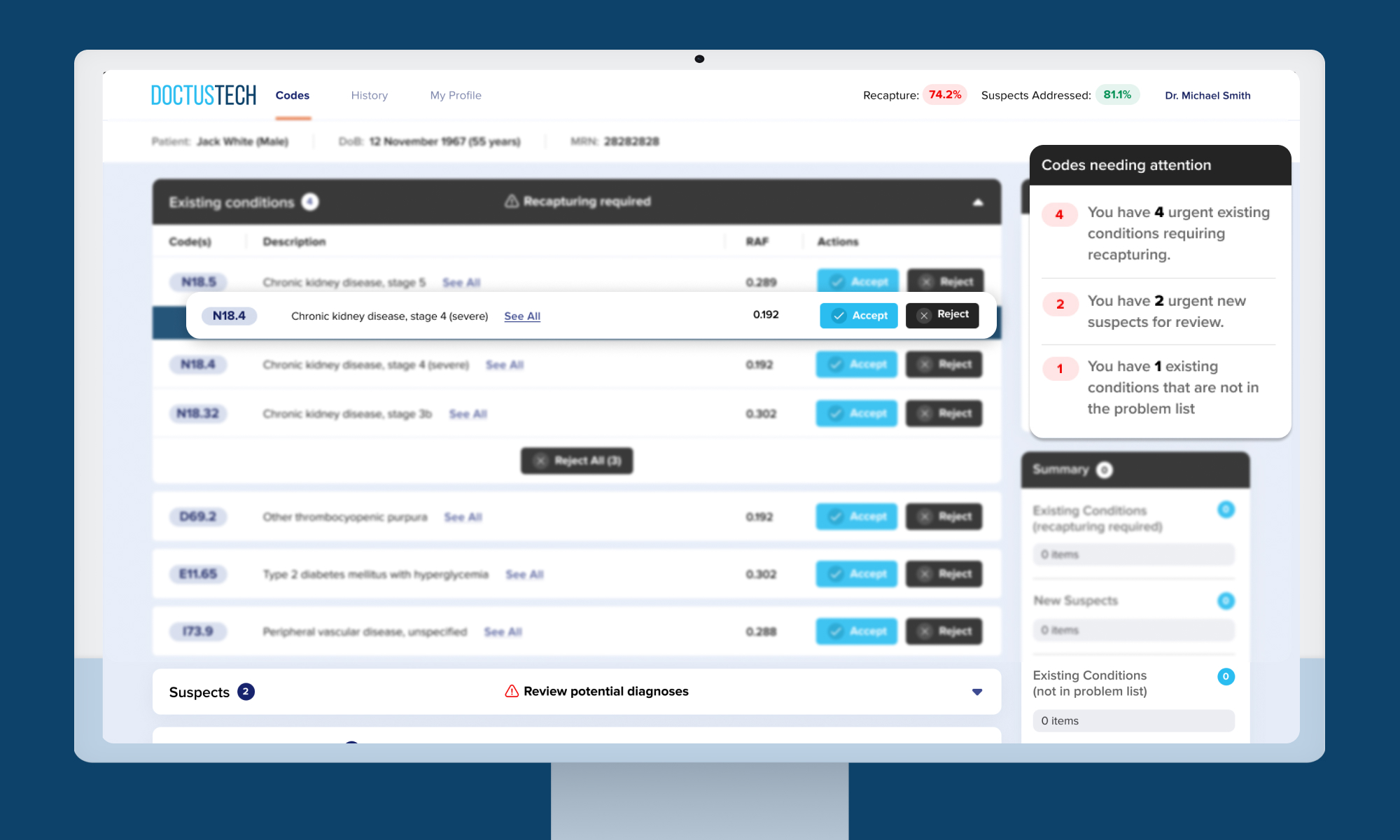
- Automated Software Solutions: AI-powered tools like the HCC Patient Diagnosis Assist Platform (PDAP) can scan clinical notes in real time to identify missing or incorrect documentation.
- Manual Chart Reviews: A team of coders or clinical reviewers can analyze records to detect patterns of under-documentation.
- Comparative Analysis: Gaps can be identified and addressed by comparing documentation trends across clinicians with similar patient populations.
The goal is to determine what is missing in the documentation—whether it’s a lack of specificity in diagnosis codes or failure to justify a condition. Without this step, feedback loops in HCC coding lack the necessary precision to drive meaningful change.
Step 2: Review & Analysis of Data
Once data is gathered, it needs to be analyzed to identify trends. Typical areas of concern include:
-
- Inconsistent documentation of chronic conditions.
- Failure to capture appropriate HCC categories.
- Overuse of unspecified codes.
- Lack of justification for diagnoses.
Software tools that integrate with electronic medical records (EMRs) can automatically highlight potential documentation errors, allowing clinicians to review and correct them in real time.
Step 3: Delivering Feedback to Clinicians
The success of this kind of initiative depends on how and when feedback is delivered. Some effective methods include:
-
- Real-Time Software Popups: AI-driven solutions can provide instant alerts when a clinician is about to close a note, prompting them to review missing or incorrect documentation.
- Personalized Dashboards: Clinicians can access their documentation performance data through an online dashboard to track their improvements over time.
- Direct Interaction: A coding specialist can provide immediate feedback after reviewing a clinician’s chart in person or through a virtual message.
For example, a hybrid model can be used where trained personnel review documentation and provide real-time interventions. This personalized approach ensures that clinicians receive immediate guidance, leading to better coding habits.
Over three months, the clinic could see:
-
- A significant increase in accurately documented conditions.
- A more consistent application of HCC guidelines.
- Clinicians reporting greater confidence in their coding decisions.
When applied strategically, real-time feedback loops in HCC Coding leads to measurable improvements in documentation accuracy.
Step 4: Justification & Training for Long-Term Improvement
Beyond just flagging errors, feedback should be educational. Providing clinicians with the reasoning behind documentation corrections fosters long-term retention. Effective training strategies include:
-
- Educational Modules: Learning apps can deliver targeted training programs based on individual documentation gaps.
- Microlearning Sessions: Short, interactive lessons can be embedded into daily workflows, reducing cognitive overload.
- Dedicated Admin Time: Some organizations allocate specific hours for clinicians to complete training and review their coding performance.
As organizations implement real-time feedback systems, they may encounter challenges that hinder the process. Let’s explore practical strategies for overcoming these hurdles and keeping the system running smoothly.
Overcoming Challenges in Implementing Real-Time Feedback
Despite its benefits, implementing such systems comes with challenges:
1. Time Constraints
Clinicians are busy, and it can be difficult to take time away from patient care to review coding errors. A well-integrated AI system minimizes workflow disruptions by providing concise, actionable feedback within the EMR.
2. Resistance to Change
Adopting new documentation practices requires behavioral change, which is often met with resistance. To counter this:
-
- Leadership should communicate the benefits of accurate coding.
- Early adopters can be identified and trained as champions to promote best practices within their teams.
- Positive reinforcement should be used, such as rewarding clinicians for improved coding habits.
3. Ensuring Feedback is Constructive and Actionable
To ensure that the real-time process is effective:
-
- Set Clear KPIs: Knowing your aim is important; it will help you monitor metrics such as condition readdress rates and documentation completeness.
- Use Comparative Data: Clinicians should see how their documentation compares to their peers.
- Follow-Up with Coaching: One-on-one guidance sessions help clinicians understand the rationale behind suggested changes.
As we explore the challenges of implementing real-time feedback loops in HCC Coding, we must recognize that different roles within the healthcare team may require tailored approaches to maximize the system’s effectiveness. While clinicians benefit from immediate insights into their documentation, other team members—such as medical coders and scribes—also play a critical role in the documentation process.
Personalizing Feedback for Different Roles
Personalizing feedback for these roles ensures that all stakeholders are equipped to contribute to improved accuracy and compliance. Let’s dive into how it can be customized for medical coders and scribes to enhance their workflows and collaboration with clinicians.
While clinicians are the primary focus, feedback can also benefit:
-
- Medical Coders: By providing real-time alerts on documentation gaps, coders can collaborate with clinicians to resolve errors before claims submission.
- Scribes: Ensuring that medical scribes input the correct information from the outset reduces the need for retrospective corrections.
As we explore the importance of personalized feedback, we must consider how technology enhances this process. Let’s look at how
The Role of Technology in Real-Time Feedback
AI and machine learning are revolutionizing HCC coding by making real-time suggestions more efficient. With tools like PDAP, clinicians can receive instant documentation recommendations, and administrators can track performance metrics and identify trends.
Additionally, the integration of the DoctusTech Learning App and PDAP allows organizations to tailor training programs to their specific documentation needs.
As we’ve seen, real-time feedback loops in HCC coding transform how clinicians and administrators approach documentation. However, the true power of this technology lies in its ability to support ongoing growth and development.
Final Thoughts: Building a Sustainable Feedback Loop
Implementing real-time processes in HCC coding is not just about identifying errors—it’s about fostering a culture of continuous improvement. Organizations that successfully integrate these systems will:
-
- Improve coding accuracy.
- Enhance patient care documentation.
- Ensure compliance with risk adjustment guidelines.
By leveraging AI-driven tools, structured training programs, and personalized feedback, healthcare organizations can create a sustainable model where clinicians continuously refine their documentation practices without disrupting their workflow.
With real-time feedback, the future of HCC coding is not just about correction but prevention, education, and long-term excellence in clinical documentation.