Clinicians and other medical staff find it hard to care about HCC coding. Here’s why they should.
Selling clinicians on the value-based care (VBC) model should be straightforward. In theory, it promises more time with patients per encounter – with a greater focus on patient outcomes when compared with the ‘numbers game’ of fee-for-service medicine. For many, VBC captures why they became doctors in the first place. But for some, the documentation requirements associated with the value-based care model stand in the way.
“The documentation is intimidating,” agrees the Chief Clinical Officer of a leading at-risk physician group. “And it wasn’t something that providers learned in medical school.” The ‘intimidating documentation’ around HCC coding is highly off-putting to providers. They don’t care about it, they don’t want to learn it, and they’d rather be spending time with patients. So why does accurate HCC coding matter, and how can we make clinicians care about it?
The problem
Physician burnout remains a major issue, and it’s clear that the accumulation of non-clinical tasks is a significant contributing factor. As an example, a recent study from the American Journal of Medicine reports that primary care physicians spend an average of two hours interacting with an EMR for every hour of patient contact – that’s 4.5 hours each day in the clinic, with an additional 90 minutes at home every evening. This quote from the same report puts the problem into context:
“I am no longer a physician but the data manager, data entry clerk and steno girl… I became a doctor to take care of patients. I have become the typist.” American Journal of Medicine
With physician burnout rates reportedly as high as 63%, it’s hardly surprising such attitudes persist. In the value-based care model, learning the intricacies of risk adjustment and maintaining accurate documentation represents another time-consuming task for clinicians. That’s why it’s so crucial that they understand and appreciate the value of accurate HCC coding.
Accurate HCC coding and reimbursement
“In addition to helping predict healthcare resource utilization, RAF scores are used to risk-adjust quality and cost metrics. By accounting for differences in patient complexity, quality and cost performance can be more appropriately measured.” – American Academy of Family Physicians
The first and most obvious point to make here is that accurate HCC coding has a direct influence on reimbursement. The risk-adjustment model depends on all risk-adjusting conditions being coded accurately – ensuring each patient has a risk score that suitably reflects their likely cost of care. Therefore, accurate coding ensures that healthcare services are appropriately reimbursed for the level of care provided to patients. In a nutshell, clinicians and other medical staff should care about accurate HCC coding because it ensures they get paid.
Inaccurate coding, meanwhile, can lead to under- or overpayment – either of which can be highly damaging to an organization’s financial stability.
Accurate HCC coding and compliance
While HCC compliance regulations can seem vague or confusing, the most common causes of audit failure include the following:
Under-documented chronic conditions
Incorrectly-recaptured acute codes
Incorrect initial encounter codes
Exclusion codes coded together
Inclusion codes missed
Accurate HCC coding, therefore, is a matter of regulatory necessity if organizations are to avoid penalties and other legal repercussions. While compliance isn’t necessarily the most powerful motivator for reluctant clinicians, it is an important reminder that accurate HCC documentation is non-negotiable for VBC organizations.
Accurate HCC coding and patient care
“Accurate diagnosis coding can help your team identify high-risk patients and give them the right care at the right time.” – American Academy of Family Physicians
This final point is likely the one that will resonate most powerfully with clinicians and other clinic and hospital staff. At its heart, the value-based care system is about reducing costs and increasing the quality of patient care.
As a part of that, accurate HCC coding helps:
Identify patients at greater risk of certain conditions or complications
Implement preventative screenings and lifestyle interventions
Minimize hospitalizations and readmissions
Ensure patients have access to the appropriate resources for their needs
Improve patient understanding and management of chronic conditions
Improve care coordination
Ensure all relevant providers have access to accurate, up-to-date information on patients’ health status
Improve quality reporting and identify areas for improvement
Accurate HCC coding is an unglamorous but essential aspect of value-based reimbursement – helping to support the fundamental promise of value-based care to improve patient experiences and enhance patient outcomes.
Improving engagement, getting buy-in
“Physician engagement can make or break a hospital’s HCC-capture strategy.” HFMA
It’s clear that accurate HCC coding is vital to the success of accountable care organizations and other VBC providers. But to code accurately, clinicians and other staff must first undergo HCC coding education. The trouble is, traditional methods of HCC training no longer work. Knowledge retention rates for ‘tired and tested’ techniques such as lectures, written materials, and demonstrations range from between 5% and 30% – which is to say nothing of the critical matter of clinician engagement.
Here at DoctusTech, we employ a revolutionary app-based learning method using a mix of multiple-choice questions and clinical vignettes. This active learning approach generates knowledge retention rates as high as 75%, and better yet, clinicians love it. Our research shows that the DoctusTech app is the preferred method of HCC education for 9 out of 10 clinicians, with an engagement rate of 90%.
If you’re struggling to get your clinical staff to care about accurate HCC coding, it’s time you tried the DoctusTech app. Schedule a demo today.
Healthcare is a dynamic and complex industry, constantly evolving to provide the best possible care to patients. In this ever-changing landscape, accurate Hierarchical Condition Category (HCC) coding and risk adjustment in the value-based care healthcare model play a crucial role in ensuring quality care, managing patient populations, and optimizing revenue. Here are 7 strategies to improve HCC coding and risk adjustment accuracy in your VBC organization.
1. Streamlined clinical workflows
Streamlined clinical workflows reduce administrative burdens and free up healthcare providers to focus on patient care. Efficient workflows can also aid in capturing HCC codes more effectively. Organizations should evaluate and optimize their workflows to ensure that providers have the time and resources necessary for accurate coding.
2. Regular coding audits and feedback
Regular coding audits are essential for identifying errors and areas for improvement. They help organizations ensure compliance with coding guidelines and enhance accuracy. Feedback from audits can guide coders and providers in refining their coding practices. These audits can be conducted regularly, and the findings should be used constructively to improve the coding process.
3. Data analysis
Data analysis is an invaluable tool in risk adjustment. By analyzing patient data, organizations can identify gaps in coding and areas for improvement. Data-driven insights can help pinpoint under-documented conditions, ensuring that all relevant HCCs are captured. This analysis also helps organizations gain a deeper understanding of their patient populations.
4. Comprehensive provider education
Healthcare providers are at the frontline of patient care, and their understanding of the importance of accurate HCC coding is paramount. Comprehensive education programs ensure that healthcare professionals are well-informed about the significance of documenting chronic conditions accurately. By equipping providers with the knowledge and tools they need, organizations can improve coding at the source.
One of the leading HCC coding education providers in this space is DoctusTech. It’s an app that clinicians can use to learn and stay updated about HCC coding. Book a demo to earn how DoctusTech helps healthcare providers train clinicians.
5. Proper documentation training
Training healthcare professionals in the nuances of proper documentation is vital. These training programs help providers understand the specific details required for accurate HCC coding. Coding specialists or educators can play a significant role in delivering this training, ensuring that providers are well-equipped to document patient conditions comprehensively.
6. Advanced EHR and documentation tools
Electronic Health Records (EHRs) have become integral to healthcare documentation. Implementing advanced documentation tools within EHR systems can prompt providers to capture relevant HCCs during patient encounters. These tools can offer real-time suggestions and guidelines, aiding providers in accurate coding.
One of the revolutionary tech solutions for improving HCC code capture is DoctusTech. It makes it easy for clinicians to accurately document HCC codes for every patient within their own EMR. DoctusTech HCC 360 streamlines EMR workflows by combining all external data sources and presenting information to clinicians as they write their progress notes. It can integrate with all major EMRs with minimal hassle. Book a demo here to learn more about this product.
7. Collaboration and communication
Effective communication and collaboration between coders, providers, and administrative staff are vital for HCC coding accuracy. Open channels of communication allow providers to seek clarification or guidance on coding, and coders to provide feedback or request additional information when necessary. This collaborative approach fosters a culture of accuracy and ensures that everyone is working together towards the common goal of improved coding.
In conclusion, accurate HCC coding and risk adjustment are essential for healthcare organizations to deliver quality care while optimizing revenue. These seven strategies – comprehensive provider education, advanced EHR tools, streamlined workflows, regular coding audits, proper documentation training, data analysis, and collaboration – collectively form a robust framework for enhancing coding accuracy. By implementing these strategies, healthcare organizations can meet the challenges of the evolving healthcare landscape while improving patient care and financial outcomes.
As the healthcare industry continues to evolve, following these 7 strategies to improve HCC coding accuracy. By investing in accurate HCC coding and risk adjustment, healthcare organizations can ensure that they are well-prepared to provide the best care to their patients while achieving financial sustainability in an increasingly complex healthcare ecosystem.
To improve your HCC coding accuracy with the DoctusTech app.
Healthcare providers and payers use the HCC coding system to identify the seriousness and severity of a patient’s medical condition. The main purpose of coding is to ensure that a patient receives good medical care and resources. If it is not performed correctly, then there will be some potential risks associated with HCC coding. Improper, incorrect, wrong, or incomplete coding could classify a patient as less sick, which could lead to inadequate care, improper payments to healthcare providers, or audits and fines and penalties paid to Medicare. Here are four key steps that healthcare providers and coders can implement to improve HCC documentation and reduce risk:
1 – Stay updated on coding guidelines
There are certain guidelines on HCC coding which can change or evolve over a period of time. It is important to stay updated with the latest guidelines, changes, and revisions. This can be achieved through regular training sessions or staying informed by reviewing resources such as CMS websites or other industry-related publications.
2 – Error-free documentation
Accurate and complete documentation is vital for HCC coding, as it properly identifies a patient’s condition and provides all the information that is needed by the patient and healthcare providers. In the end, all the relevant diagnoses, procedures, and treatments should accurately reflect the patient’s conditions in the coding document.
3 – Regular audits
Conducting regular audits is crucial to identifying potential errors and correcting them, and to avoid penalties, so that patients get the proper treatment. Regular audits can be implemented by internal staff or by third-party auditors. This includes a review of accuracy, documentation, and compliance requirements.
4 – Leveraging the technology
There are numerous online tools available which can help in HCC coding, these include coding software, EHR systems, and other electronic tools. These instruments can facilitate coding, lessen errors, and help in maintaining the consistency among different coders and providers.
Potential risks can be avoided by staying updated on current coding guidelines, changes, and compliance requirements. This will help to improve the quality, reliability, and accuracy of HCC coding. It is an important factor that reflects a patient’s health status and ensures he/she receives proper care and resources.
To know more about the list of HCC codes, you can also read our blog on “What Is HCC Coding ?“
With the flu season ramping at unprecedented rates, and a new surge of RSV coming when COVID-19 numbers are rising again, the topic of a healthcare surge emergency is back in the headlines. What the New York Times is calling a “Tripledemic” is threatening to overwhelm providers and hospitals yet again. During the peak of the pandemic, hospitals experienced a surge in demand for physical resources and personnel that lasted nearly two years. And just when things started to adjust back to some recognizable norms, the question is again on everyone’s mind: “How do we tackle a surge?”
According to Shereef Elnahal, MD, president and CEO of University Hospital and former Commissioner of New Jersey’s Department of Health, hospitals and health systems often lose money during their peak seasons. Supply shortages are largely due to the fact that most hospitals use a fee-for-service payment model.
Hospitals that charge on a fee-for-service basis are paid based on the volume of patients they treat, not the quality of patient outcomes. Because of this, hospitals usually operate at full capacity in order to reap the greatest rewards. When patient volumes rise during peak seasons, however, hospitals have little margin for error.
According to static payment rates for inpatient care, hospitals may struggle with seasonal demand. In order to keep up with surges, health systems may have to hire more staff or order more supplies, which leads to increased expenses despite no increase in revenue.
During flu season, primary care physicians often augment their workforce by up to 30 percent and still face financial challenges and capacity limitations. Across all healthcare facilities, staffing shortages have become worse as a result of the COVID-19 pandemic, which increased the need for healthcare professionals.
Rather than relying on simply adding more headcount, health systems needa model that can easily adjust healthcare delivery to fit any situation, including increased patient capacity and pandemic surges. Creating a value-based payment model may give health systems more flexibility when dealing with demand surges.
According to the quality of care, providers are compensated using value-based payment models, not the quantity. This approach may inspire health systems to improve staffing procedures. In contrast to dividing physicians’ time in a way that will lead to the highest number of completed services, health systems might focus on patient needs and health outcomes in order to address them.
Physicians using a value-based model are less likely to refer patients to specialty care facilities if those referrals are not medically beneficial.
Because of Maryland’s value-based all-payer model, which reimburses hospitals using global budgets for inpatient episodes of care, hospitals in the state were able to manage the influx of patients during the pandemic far better than neighboring states with different models.
A study from JAMA Network Open noted that the all-payer model also decreased surgical spending and surgical complications. Providers can save resources and supplies for busy periods if they are reimbursed based on outcomes rather than quantity of services.
Patients may be able to avoid expensive hospital stays, saving staff time and resources, if they have access to healthcare services at home. Hospitalization rates may also be lowered by using home-based primary care services.
In addition, health systems could leverage telehealth services to assess patients and determine if an in-person visit is required. According to the authors, telehealth use could improve access to care and save hospitals money.
Patients may also be able to manage their acute conditions from home using remote patient monitoring technology.
Surges can also be a contributing factor to physician burnout. That is why reducing physician workload (blog post) should be a part of hospitals’ strategy of dealing with patient surges.
The DoctusTech Mobile App is based on our successful HCC education and retention strategy, which relies on clinical vignettes customized to the clinicians’ weaknesses and strengths, which are sent to their mobile phones every week. With an engagement rate of 90%, DoctusTech App results far exceed any other learning tool, technology, or strategy.
After using the app for HCC coding education, clinician RAF accuracy is consistently increased based on the learning data.
What methods does the app use to accomplish this?
Our app gamifies the learning experience, connects clinicians with one another, allows them to compete for real prizes, and provides administrative support. In addition, the most advanced HCC code search tool in the world is available. Clinicians earn 25 CME hours every year as they learn HCC coding in a non-boring app!
Audits are no longer just for large payors, provider groups are feeling the pressure of rising compliance audits, and the playing field is complicated to negotiate. Some of this may seem unfair, but with the cost of medical fraud on the rise, the DOJ, CMS, OIG, HMS and all the other initials are not going to let up any time soon, if ever.
The DOJ sued Cigna in October, the Supreme Court refused to intervene on behalf of Molina Healthcare’s whistle-blower case, and more negative audit and antitrust cases are appearing daily.. You may be doing your best but that is no defence in an audit. The only things that matter are facts, documentation, accuracy, and pure compliance. Practicing medicine is an art, but documenting is a strict science, and anything less than precise documentation may result in poor audit outcomes and your company’s name up next in the headlines.
The DOJ is relentless, but not unpredictable. It turns out, they consistently target the same set of codes in nearly every suit. Apparently, the “low-hanging fruit” can be bucketed into four simple categories: Acute coded as chronic; Lack of clinical accuracy or supporting documentation (MEAT Criteria); and Diagnosing without changing the plan of care.
We’ve pulled together a list of “The Usual Suspects” – HCC codes that appear most frequently in DOJ audits, and married the specific codes with strategies to both find them in your EMR and avoid them in your coding. Access the most common offenders in our free report.
Back in 2004, CMS introduced HCC coding as a tool to help estimate Medicare costs. Today, HCC coding us used across Medicare Advantage plans, the Medicare Shared Savings Program, Medicaid, and private health plans – all deploying a variation of the risk adjustment model in order to quantify the upcoming cost of care for their member population, and as a mechanism of submitting that care need to CMS for payment. And yet, the question comes up more often than you may think: “What is HCC Coding?”
Even in the value-based care space, there is confusion around HCC coding, which ICD10 codes risk adjust, and how to diagnose and document accurately and specifically. So if you’re moving from fee-for-service into VBC, taking on risk for the first time, or a veteran at HCC coding for VBC, this article will clarify much of the confusion and simplify what HCC coding is, why it matters, how it is used and what the future holds for HCC and VBC.
Do Doctors Know HCC Coding?
First, clinicians typically have a good working knowledge of ICD-10 codes. And every org has their lookup functions baked into the EMR. However, not only do most ICD-10 codes not work as HCC codes, many of the traditional ways of diagnosing in the fee-for-service world are turned on their heads in VBC. So knowing or having access to ICD-10 codes is not actually that much of an advantage when learning HCC coding. In fact, in some cases, that knowledge can be a liability.
Knowing the code to document diabetes is great, but using that same basic E11.9 that you’re used to is not helpful when diagnosing in a risk model. You need to dig into the complications, the severity of the disease state, and both diagnose and document with high specificity in order to treat and afford to treat the full complications of the disease. If you under-diagnose, you will likely under-treat, and risk an avoidable hospitalization, the risks to the patient and the costs notwithstanding. So in the case of diabetes, a quick check of the toes could yield a missed diagnosis that is critical to the patient’s care as well as accurate RAF and adequate capitation.
What are HCC Codes?
Hierarchical Condition Categories – as the name implies, the categories relate to a hierarchy of of conditions, and it all works together as an efficient sort function to calculate the risk that the patient’s will be expensive. Think about it like this: A patient with mild diabetes as unlikely to end up in the ER due to their disease, so basic diabetes does not risk adjust; whereas a patient with severe diabetes with complex circulatory symptoms that have already led to amputation of one toe is at extremely high risk of ending up in the ER, and they will require a lot of personal and intense care to keep them out of the hospital. And care costs money, so risk and care are nearly synonymous. A higher risk diagnosis gets an HCC code with a higher risk adjustment score, which adds a higher multiplier to the capitation of that patient – meaning the government pays more dollars a month to maintain that disease and help that patient stay out of the hospital.
How do clinicians use HCC coding?
The primary use of HCC codes is to document new chronic condition diagnoses, and recapture chronic conditions being treated, and communicate those diagnoses to Payors and CMS in order to receive capitated payments.
How do HCC codes translate to revenue?
The payment model is obviously vastly different from the traditional fee-for-service (FFS) format where actions are performed, justified, transmitted as CPC codes and reimbursed by payors and/or CMS. In the VBC model, a patient is diagnosed with a specific chronic condition, that condition is documented and coded based on hierarchical condition categories that adjust the risk associated with keeping that patient healthy and out of the hospital. By taking on that risk, the plan or provider group is agreeing that, if given a reasonable amount of money, they will be able to maintain the health of that patient. That money directly ties back to the HCC codes documented, and is paid on a capitated model, with a certain dollar amount paid per-member per-month (PMPM). Those payments allow the overall organization to provide excellent care to the entire patient population, paying extra attention to those whose disease states have reached a complexity where significant resources are required to maintain optimal health. Whether for-profit or non-profit, the organization providing care will financially benefit from accurate diagnosis coding and aggressively proactive care.
How does HCC coding help doctors get paid?
When done correctly, practicing medicine in a Value-Based Care arrangement means more time for doctors, less administrative burden, less burnout and more time to spend per-patient. Smaller panels, and more help treating patients mean that a good doctor can provide truly life-changing care to patients without over-working or over-coding. And by practicing good medicine with proper HCC documentation, you will find your organization flourishing and your patient outcomes improving – all while actually decreasing the overall cost of healthcare. Sure, there is no such thing as a perfect system, but this is as close as we can get in today’s environment. And with an eye to continuous improvement, good coding and good care puts your organization squarely on the path.
How does HCC coding translate to patient care?
You cannot treat what you do not diagnose. And if you diagnose with an eye to changing the trajectory of the patient’s care plan, you are practicing good medicine. To diagnose without proper documentation denies the patient the care that comes from critical revenue. And to document without care is, simply put, fraud. So diagnose with high specificity and proper documentation to ensure that your clinic can afford to provide the kind and quantity of care that will keep your VBC patients out of the hospital. Better HCC coding = better care.
How long does it take to learn HCC coding?
Depending on the tools used for teaching and learning, it can be a years-long process fraught with frustration and difficulty – OR – it can be a simple weekly check-in on an app that uses modern learning methodologies to make mastery quick and easy.
How does HCC coding relate to compliance audits?
The number of compliance audits of provider groups has been steadily rising. The DOJ launches new lawsuits against both large payors and smaller provider groups with increasing penalties. And the Supreme Court has refused to step in and ease the pressure, letting whistle-blower cases proceed unchecked. Clinicians are doing their best, but that is no defense in an audit – the only thing that matters is facts, documentation, accuracy and pure compliance.
Practicing healthcare is an art, but documenting is a strict science, and anything less than accurate documentation vigorously maintained will likely result in negative audit outcomes and your group’s name landing in next month’s headlines.
CMS and DOJ have been increasingly scrutinizing payor strategies and billing patterns as it pertains to Hierarchical Condition Categories (HCCs). As more and more physician groups take on risk in the VBC models, it is imperative that physician groups do not make the same mistakes as their payor partners (intentionally or not).
Some of the most common offenses are fairly simple to avoid. But as we all know, simple does not mean easy. In fact, achieving simplicity can be far more difficult than creating complexity – which is what happens most of the time. A simple solution requires tremendous discipline.
HCC coding for acute conditions
As a rule of thumb, an acute code should not repeat 2 years in a row for a specific patient. And usually, even the first year is inaccurate. Acute heart attack is one of the most common errors penalized by CMS and the DOJ. One reason for this is misunderstanding how to document “history of heart attack” vs “heart attack.” Another version is chronic conditions that have been mis-coded as acute. There is a very short distance between upcoding and practicing good medicine.
It is sometimes appropriate to use these within the year where the acute event occurred, but the following year you must diagnose and document a different code. A third of the most common acute condition dinged by CMS is the combination of #1 & #2 – Acute Stroke and Acute Heart Attack.
Lack of clinical accuracy or supporting documentation – Medical diagnoses are complex and sometimes exist in the gray area between possibilities – but coding and compliance are hard rules. Picking the wrong code. Commonly misused diagnoses. While RADV audits are routinely looking for MEAT criteria, they’re not looking for clinical criteria or diagnostic accuracy.
Commonly misrepresented diagnoses: The exact criteria can be confusing even though the treatment can be the same for mild, moderate, and severe forms of certain diseases. Misrepresentation of the severity can result in overpayment from CMS, and legal and financial penalties – not to mention the obvious ethical concerns.
What is HCC Coding Without Plan of Care?
Now that a doctor has diagnosed a chronic condition, what is the plan to treat or manage the disease? A diagnosis that does not demonstrate a direct and deliberate impact on the plan of care is almost always incorrect at best, and in an audit, illegal. Diagnosing and documenting should function as a mechanism of providing care; documenting to document is never correct. So be on the lookout for conditions diagnosed and codes submitted that do not impact the plan of care. These are often targeted by CMS, both in OIG compliance audits and RADV audits.
How is HCC Coding improved by Education and 1-on-1 coaching?
Build a culture that connects patient care to diagnostic specificity and accuracy in coding and documentation. No doctor wants the business managers coming down from their offices, clipboard in hand, scolding about how code capture and RAF scores impact revenue. But every clinician understands the need to improve care and decrease cost. So start there – in VBC, practicing good medicine and providing better care starts at accurate diagnosis right through to rigorous documentation.
Documentation enables treatment, funds resources to provide care, ensures better health outcomes for patients and actually lessens clinician workload – when done correctly. Chart audits do not have to be brutal, they can be helpful, asking clinicians how a particular diagnosis changes the care trajectory, and helping document for maximum patient benefit. Internal meetings should focus on coding as care. And manual chart reviews should be performed by medical doctors to give timely 1-to-1 feedback. If this is done, the last error on the OIG’s list of usual suspects will go down:
How does HCC coding impact clinician workload?
It can go either way – with increased coding requirements becoming a burden, both to learn in boring seminars and to chase down in chart reviews. But with modern advanced app-based learning tools like DoctusTech, clinicians can master HCC coding in as little time as 5 minutes per week.
What is HCC coding to the OIG?
The Office of Inspector General of the Department of Health and Human Services is at the forefront of auditing healthcare fraud, and recommending action from the DOJ.
From OIG: Since its 1976 establishment, the Office of Inspector General (OIG) has been at the forefront of the Nation’s efforts to fight waste, fraud and abuse and to improving the efficiency of Medicare, Medicaid and more than 100 other Department of Health & Human Services (HHS) programs.
In today’s healthcare landscape, the OIG is finding value-based care to be a target-rich environment, with special focus placed on Medicare Advantage programs, as these allow a small action (documenting a chronic condition that does not actually exist) to multiply into a year of capitated payments to an organization. The simple act of up-coding a condition into something more complex than it should be or over-coding by documenting a chronic condition that does not exist results in thousands of dollars per year in fraudulent overpayments.
What is HCC coding to the DOJ?
While the Department of Justice is not directly concerned with healthcare, they are very concerned about medical fraud, which defrauds the government’s medicare programs, and in extension, the American people. Most often, the DOJ takes on whistleblower cases, where an individual from inside an organization shares insider information regarding acts of upcoding or overcoding that are both large and systemic. These whistleblowers stand to profit significant sums, at times earning up to 20% of the total settlement. And with the recent Sutter case settling at $90,000,000, the whistleblower could potentially take home $18 Million. The False Claims Act ensures that the federal government has a means of penalizing organizations and individuals who, through filing false claims, defraud the government. While this law has been in place since the 1800s, it is getting renewed attention as the DOJ discovers millions of dollars in false claims specifically in Medicare Advantage programs, as these allow an organization to bill CMS with very little scrutiny or oversight.
Top mis-used HCC codes
We address this in a report, feel free to request it HERE.
Also, codes most found in unlinked chart reviews, and subject to RADV audits are detailed in our white paper, found HERE.
What are the requirements for HCC coding documentation?
Generally referred to as the MEAT Criteria, here are the four things you must have to document an chronic condition with an HCC code:
M = Monitoring by ordering or referencing labs, imaging studies or other tests
E = Evaluation with a targeted part of the physical examination specific to a certain diagnosis
A = Assessment of the status, progression or severity of the diagnosis
T = Treatment with medication, surgery, lifestyle modification, or referral to a specialist.
What are the best HCC coding tools?
What apps are available for learning, search, lookup, documentation? This may be a bit of a self-promoting softball, but if you haven’t checked out the DoctusTech app by now, you really should. Make time with a member of our team to see if the DT app is right for your team. Demo DoctusTech today.
What is the best way to change physician behavior around HCC coding
Notes and insights from a study published by AJMC on how to change physician behavior. “The authors evaluated methods for implementing clinical research and guidelines, in order to change physician practice patterns, in surgical and general practice. They evaluated the effectiveness of different implementation methods.”
And as we have demonstrated through successful behavior change in physicians using our HCC coding education app, the most common solutions aren’t the most effective when it comes to ongoing positive change in physician behavior. Want to learn how to change physician behavior? Let’s dig a little deeper into a review of reviews, revealing some hard truths.
We’ve been saying for years, lectures do not work. Emails do not work. If you want to know how to change physician behavior on HCC coding, don’t take our word for it. The American Journal of Managed Care released a systematic review evaluating fourteen medical reviews in an effort to understand which interventions are most effective in changing physician behavior for the better and improving patient outcomes.
It is evident from their publication that the methods of intervention most commonly deployed in teaching doctors HCC coding are rarely able to create lasting change in physician behavior.
What is the best tool inside the EMR?
The DoctusTech Patient Data Analysis Platform (PDAP) is the premier tool for Value-Based Care, living inside the EMR and helping clinicians find and use the best HCC codes, track and manage care associated with chronic diagnoses, and learn which codes to use for which patients – all while reducing clinician workload. It helps readdress conditions diagnosed last year, significantly improving recapture rates. And it helps administrators see into the data by clinician, patient, clinic or by codes. Learn how the DoctusTech PDAP can help your patients and your doctors live happier, healthier lives. Demo DoctusTech today.
Value-Based Care is a natural movement toward the benefit of the patient with a reduction in costs by aligning all incentives in the right direction. And as providers make the shift, patients will be encouraged both by the motive behind the transition as well as the improvement in their overall health and the reduction in the costs of their care. Truly, Value-Based Care has the potential to be a significant win-win for patients and providers. And in the end, isn’t that why you spent all those years pursuing your medical training? Value-Based Care is for patients, and for the providers who care for them.
The market is now moving towards building value-based care drivers to all types of patients outside of Medicare Advantage. It’s unlikely a brand new risk model will be born for commercial patients. Therefore, all physicians will need to understand the risk adjustment models and the implications of documentation accuracy for reimbursement.
Why is HCC Coding Important for Value-Based Care?
HCC coding’s importance is less about the impact on revenue and more about the shift towards VBC models, which have consistently shown better clinical outcomes at lower costs. And Hierarchical Condition Category Coding is the language clinicians use to document the diagnoses of chronic conditions and the complications and various disease states that contribute to risk.
Why should doctors care about HCC coding?
Doctors should, first and foremost, care about patients – and they do. But as a mechanism of that care, doctors must diagnose with specificity and document with accuracy in order to provide care and the revenue that affords that care. And HCC coding is how that is done. HCC coding is the documentation foundation for most of the value-based care arrangements used today. With “value-based care” usually being equated with Medicare Advantage, in coming years we believe that VBC will be incorporated into nearly all types of financial models.
HCC coding falls under the broader term of Risk Adjustment (RA) models for prospective payment. These models are designed to determine risk scores and assign a fee according to the patient’s level of risk.
In the Medicare Advantage world, these models use certain demographic and HCC codes to assign a risk score to patients known as an RAF. The assumption is the sicker the patient, the higher the RAF, the more dollars it will take to care for this patient during any given year. Therefore the RAF score of any patient population will determine the prospective payment Medicare disburses.
This prospective payment model based on RAF does 2 things:
Aligns physician incentives. Currently, clinicians make money from taking care of sick patients. The sicker the patient, the more visits, tests, surgeries they have to do, and the more they are reimbursed. In this model, clinicians are incentivized to keep patients healthy and therefore require LESS tests and surgeries.
Spurs clinical innovation the right way. Right now, pharmaceuticals and medical hardware companies are all trying to find ways to treat diseases. The newer the drug or medical device, the more revenue they make. In this model, healthcare groups are incentivized to find new ways of preventing the disease progression from ever needing the latest drug or newest medical surgery equipment.
How can DoctusTech Help?
We provide a modern learning tool for the modern clinician, using gamification, competition, real prizes and administrative oversight to see who is engaging and who needs a little extra help. Also, our app deploys all the subtle nudges and complete with the most advanced HCC code search tool on earth.
DoctusTech helps clinicians learn HCC coding through clinical vignettes in an app that is fun and engaging. Diagnosing with the appropriate HCC code is a critical skill for modern clinicians who care for patients in a value-based care arrangement.
You cannot treat what you do not accurately diagnose, and you cannot afford to treat what you do not appropriately code. Without the correct diagnoses and accurate documentation and coding, caring for patients with complex disease will be unsuccessful, leading to increased avoidable hospitalizations and increased cost to the organization.
In December of 2021, the Mayo Clinic published an alarming report: ⅓ of physicians surveyed intended to reduce their work hours – that represents 336,000 doctors. While—and I hope you are sitting down—1 in 5 physicians intended to leave their practice altogether – 20%, or 204,000.
The cause? Burnout.
Burnout from workload, COVID-19–related anxiety/depression, and fear of contracting the disease. Now, some of those burdens have certainly eased over the past 10 months – but the prevailing concern of burnout from overwork has hardly abated.
Burnout is a widespread problem in any industry, but the stakes are even higher in healthcare with lives of patients on the line. Quality and safety of care is our top priority and errors or lack of awareness can lead to terrible consequences.
With burnout on the rise and VBC/HCC knowledge requirements continuing to grow, it can feel like there is an impossible riptide in front of today’s clinicians. And with healthcare relentlessly marching in the direction of Value-Based Care, it’s no wonder why new clinicians have a difficult time onboarding. Requiring providers to add HCC coding to their already complex workflow is not only vital to improve the industry, it is increasingly mandated by CMS.
The DoctusTech HCC Coding App is designed with a sole purpose in mind: to reduce clinician workload, and make it easier for them to diagnose, and ultimately, take care of their patients.
The Socratic method, clinical vignettes, and question and answer sessions are the most effective methods for capturing long-term knowledge. This is how doctors were taught in the first place, and this is the best way to do it. With DoctusTech, they can learn HCC coding in the same manner—from other doctors using clinical vignettes—on their own time, requiring only an average of five minutes per week.
The DoctusTech Mobile App is based on our successful HCC education and retention strategy, which relies on clinical vignettes customized to the clinicians’ weaknesses and strengths, which are sent to their mobile phones every week. With an engagement rate of 90%, DoctusTech App results far exceed any other learning tool, technology, or strategy.
After using the app for HCC coding education, clinician RAF accuracy is consistently increased based on the learning data.
What methods does the app use to accomplish this?
Our app gamifies the learning experience, connects clinicians with one another, allows them to compete for real prizes, and provides administrative support. In addition, the most advanced HCC code search tool in the world is available. Clinicians earn 25 CME hours every year as they learn HCC coding in a non-boring app!
If HCC Coding and Physician Burnout are at all on your radar, we’d love to share a solution to both. Better solutions are out there – and they outperform seminars and code-of-the-month email blasts for engagement and results. And they free up your coaches to focus on the 20% that need it the most.
HCC coding accurately estimates future healthcare costs while improving patient care. But like any other tool, it’s only effective if the people who use it master it.
Without comprehensive education, even the most advanced coding tools can fall short. That’s where DoctusTech comes in, providing the support and resources to help your organization implement HCC coding education effectively.
In this article, we will share how you can use our learning app to deploy HCC coding education across your organization.
Empowering Your Team with HCC Coding Education
At DoctusTech, we are always eager to assist healthcare organizations in boosting HCC training programs. Our unique approach, which focuses on solving the three shortcomings of risk adjustment—the data gap, the workflow gap, and the knowledge gap—is critical and sets us apart from other solutions.
Most available solutions address only the data or workflow gaps. However, if your clinicians don’t have the right knowledge, you won’t obtain the outcomes you desire, no matter what you do to resolve the data and workflow issues. We strongly believe that if you resolve HCC coding knowledge challenges, you will also fix your data and workflow issues along the way.
The DoctusTech Mobile App is designed based on our successful HCC education and retention strategy, which relies on clinical vignettes customized to the clinicians’ strengths and weaknesses, sent to their mobile phones weekly. With a 90% engagement rate, the DoctusTech App’s results far surpass any other learning tool, technology, or strategy.
According to the learning data, we consistently increase RAF accuracy after they start using the app for HCC coding education.
How Does DoctusTech Mobile App Achieve This?
Clinicians can use our app to gamify their learning experience, engage with their peers, compete for real prizes, and receive administrative support. Our app also comes with the most sophisticated HCC code search tool available. In addition, clinicians earn 25 CME hours every year as they learn HCC coding in a non-boring app!
Also, our app offers weekly, personalized training that provides valuable insights about the clinicians’ progress.
This data-driven approach helps identify knowledge gaps, enabling more focused coaching for continuous improvement and ensuring your team is always growing and learning.
Clinical Vignettes – The secret sauce!
Most doctors who have just graduated from medical school or residency programs know little to nothing about coding for risk adjustment and value-based care. In the past, these clinicians were forced to sit in seminars and learn the correct codes to diagnose and document them properly.
Every other important medical fact is learned in clinical vignettes, so clinicians have difficulty retaining and applying information learned in boring seminars or email blasts. Simply put, incorporating new HCC codes into daily practice is hard – which is why the DoctusTech HCC coding education app is so vital.
Doctors prefer to learn using the Socratic method, clinical vignettes, and question-and-answer sessions because it is the most effective way to capture long-term knowledge gain. This is how doctors are educated, and this is the best way.
DoctusTech enables them to learn HCC coding in the same manner—from other doctors, using clinical vignettes on their own time, requiring only an average of five minutes per week.
Get in touch to learn more about how DoctusTech helps!
DoctusTech helps clinicians learn HCC coding through clinical vignettes in an app that is fun and engaging. Diagnosing with the appropriate HCC code is a critical skill for modern clinicians who care for patients in a value-based care arrangement. You cannot treat what you do not accurately diagnose, and you cannot afford to treat what you do not appropriately code. Without the correct diagnoses and accurate documentation and coding, caring for patients with complex disease will be unsuccessful, leading to increased avoidable hospitalizations and increased cost to the organization.
And without a tool to get clinicians quickly up to speed on diagnosing for risk at the point of care, coding accurately and documenting correctly, you will be stuck. Stuck in boring seminars that rarely affect lasting behavior change; stuck with missed diagnoses and missed revenue targets; stuck with patients missing out on essential care; stuck with overworked clinicians; stuck.
How do clinicians learn HCC coding?
This is where DoctusTech Helps. We provide a modern learning tool for the modern clinician, using gamification, competition, real prizes and administrative oversight to see who is engaging and who needs a little extra help. Also, our app deploys all the subtle nudges and complete with the most advanced HCC code search tool on earth.
And clinicians earn 25 hours of CME per year, while they learn HCC coding in a non-boring app!
In SCUBA diving, the diver must add just the right amount of weight to maintain perfect positive buoyancy; too much and you will sink, too little and you will bob on the surface like a cork. Risk adjustment in value-based care has some similarities: a successful VBC program will diagnose and treat just the right conditions. Not over-coding, and not under-diagnosing.
Clinicians learn HCC coding better in clinical vignettes
And doctors coming out of medical school and even residency programs know little to nothing about HCC coding and diagnosing for Risk Adjustment and Value-Based Care. Traditionally, these clinicians sit in seminars getting force-fed codes in an effort to teach them how to accurately diagnose and document with the appropriate HCC codes. Unfortunately, this is not how every other vital piece of medical information was learned, so clinicians struggle to retain the information and utilize it in daily practice.
Medical education is all about the Socratic method, question and answer, clinical vignettes. Doctors learned to learn this way, and they prefer it. Which is why DoctusTech helps doctors learn HCC coding the way they like to learn – from other doctors, in clinical vignettes, on their own time, and in an average of 5 minutes per week.
Truly, DoctusTech helps clinicians learn HCC coding. And when clinicians master diagnosing for risk with HCC codes, your whole VBC program improves.
See more ways that DoctusTech Helps:
DoctusTech Helps: Increase RAF Accuracy
DoctusTech Helps: Decrease clinician workload
DoctusTech Helps: Deploy HCC coding education across your org
As the U.S healthcare system transitions towards value-based payment models, independent clinicians and physician groups continue to face HCC coding challenges that not only impact their bottom-line, but patient care as well. On top of all this, the pandemic has added a significant burden to the already stretched clinician workload.
Here are 4 key HCC coding challenges clinicians are facing now, and how they can overcome them.
Physician training for HCC coding – Physicians are already working tirelessly to provide excellent care to their patients. Asking them to learn HCC coding through brute-force via zoom calls, classroom seminars and email blasts is a bridge too far. On the other hand, the focus on value-based care has made it imperative for physicians to know and understand HCC coding so that they can accurately document patient records. So clinicians know they need to know, they just don’t have an effective and engaging mechanism for efficient and effective learning.
Revenue impact due to incorrect coding – Accurate HCC coding is necessary for accurate reimbursements and patient care, and inaccurate coding can directly impact the bottom line. That is why it is imperative that clinicians and staff be well trained in HCC coding. And the complexities don’t stop there. HCC codes not only impact RAF scores, they also interact directly with patient care, and a fair level of decision support is required , as HCC codes are not intuitive.
Poor HCC integration with EMR systems – When HCC coding does not integrate with the EMR, it creates a complex struggle for clinicians and physician groups. This not only leads to unintentional errors, but makes workflows more difficult and adds to the burden of an already heavy workload. It is critical to put a system in place that teaches clinicians to accurately document HCC codes on every patient, and integrates within the EMR.
Lack of trained HCC coding professionals – Staffing shortfalls not only plague small practices, but larger physician groups are short-staffed as well. A lack of well-trained staff may be related to revenue or rising salaries, which sometimes small practices are unable to sustain. And when larger hospitals acquire smaller practices, a shortage of trained staff is often just one side-effect. Training clinicians and non-clinical staff on HCC coding is vital.
Transitioning to a value-based care model will never be seamless until these challenges are solved. How? With our unique suite of HCC education and EMR integration tools, enabling physicians to learn HCC coding and integrate an AI-powered HCC coding system into their existing EMR platforms to drive efficiency and accuracy.
To learn how our HCC coding app lets physicians train for HCC coding click here.
To understand how our EMR integrated platform works, click here.
As healthcare continues shifting from fee-for-service (FFS) to value-based care (VBC), accurate documentation and coding have become more critical than ever. Hierarchical Condition Category (HCC) coding is at the heart of this transition.
In this article, we’ll explore the fundamentals of HCC coding, how it impacts reimbursement, and why providers—even those outside of VBC—should take notice.
What is HCC coding?
HCC stands for hierarchical condition category. It is a risk-adjustment coding model exclusively designed to estimate future healthcare costs for patients. The process of HCCs medical coding started in 2004, but it recently gained popularity due to payment models shifting from fee-for-service (FFS) to value-based care (VBC) arrangements.
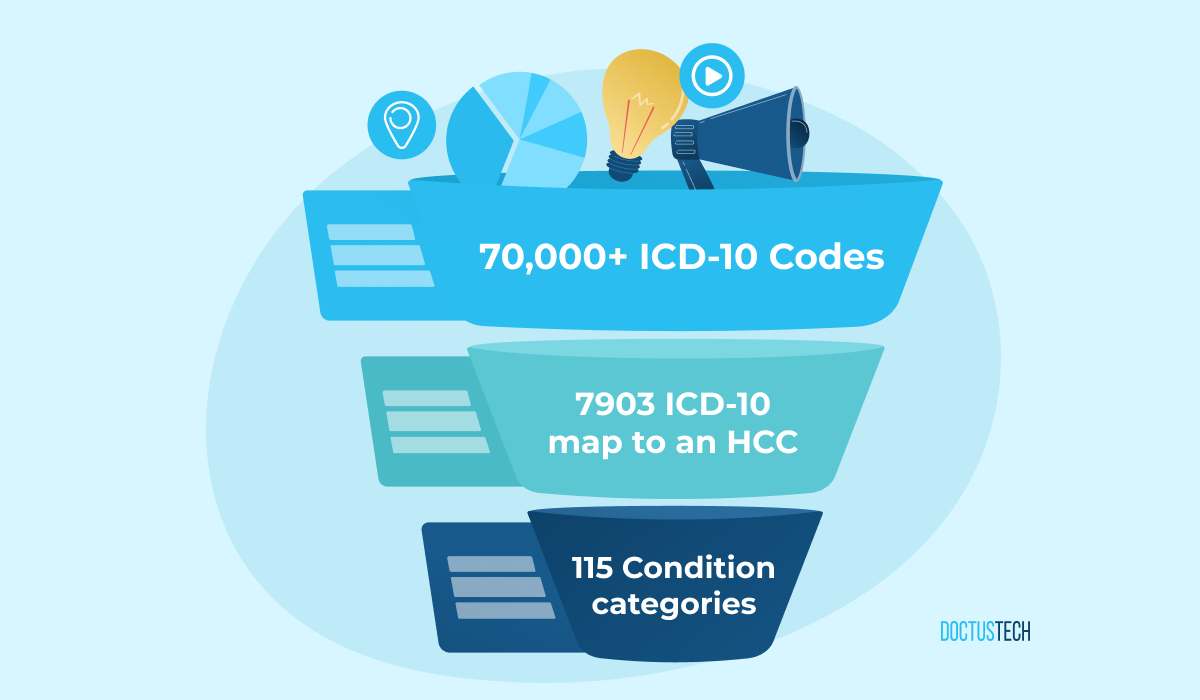
Fig 1. Out of 70,000+ ICD10 codes, 7903 ICD-10s map to a hierarchical condition category. Each HCC ICD10 is subsequently bucketed into 115 individual “condition categories.
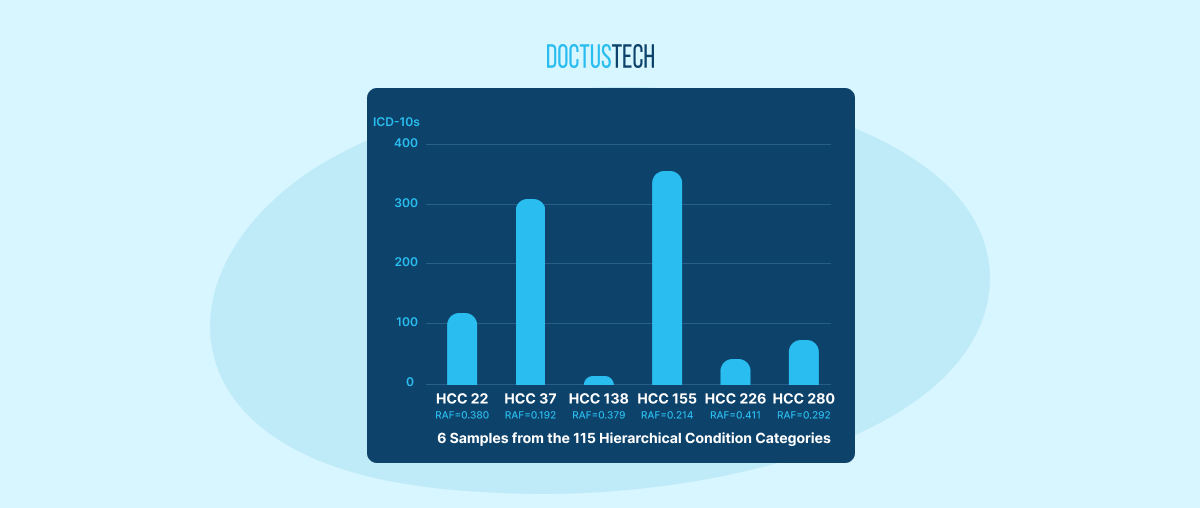
Fig 2. Each of the 7903 HCC codes is put into one of 115 condition categories. Each condition category carries a specific RAF. No matter how many ICD10 conditions a patient has in the same category, they will only be assigned the RAF score one time
Medicare assigns a risk score known as a risk adjustment factor (RAF) to each of the 86 individual condition categories. RAF scores of patient populations are subsequently used by Medicare and other payors to predict the cost of care, which influences reimbursements.
For the remainder of this article, we will explore the rationale behind HCC coding and why all providers (even those NOT in a value-based care arrangement) should care.
Why should doctors care about HCC coding?
HCC coding is the cornerstone of most value-based care arrangements. Today, “value-based care” is used synonymously with Medicare Advantage, but in the near future, we believe all forms of reimbursement will be tied to some VBC arrangement.
HCC coding falls under the broader term of risk adjustment (RA) models, where patient care is paid based on a prospective payment model. Specially designed RA models are used to determine risk scores for patients. In the Medicare Advantage world, these models use the demographics and HCC diagnoses of the patient to assign a risk score known as an RAF. The assumption is that the sicker the patient, the higher the RAF, and the more dollars it will take to care for this patient during any given year. Therefore, the RAF score of any patient population will determine the prospective payment Medicare disburses.
This prospective payment model based on RAF does 2 things:
1. Aligns physician incentives. Currently, clinicians make money from taking care of sick patients. The sicker the patient, the more visits, tests, or surgeries they have to do, and the more they are reimbursed. In this model, clinicians are incentivized to keep patients healthy and, therefore, require fewer tests and surgeries.
2. Spurs clinical innovation the right way. Right now, pharmaceuticals and medical hardware companies are all trying to find ways to treat diseases. The newer the drug or medical device, the more revenue they make. In this model, healthcare groups are incentivized to find new ways of preventing the disease progression from ever needing the latest drug or newest medical surgery equipment.
As Medicare and payers alike are starting to take notice of #1 and #2 above, the market is now trending towards building in value-based care drivers to all types of patients outside of Medicare Advantage. It’s unlikely a brand new risk model will be born for commercial patients. Therefore, all physicians will need to understand the risk adjustment models and the implications of documentation accuracy for reimbursement.
Conclusion
HCC coding is here to stay and will only grow in the years to come. While the market has heavily leveraged medical coders or third party vendors to do much of the lift thus far, V2 of Value-based Care will require all clinicians to understand and participate in it for every patient visit.
HCC coding’s importance is less about the impact on revenue and more about the shift toward VBC models, which have consistently shown better clinical outcomes at lower costs.
HCC (Hierarchical Condition Category) coding is a risk adjustment model used in healthcare to predict future medical costs for patients. It categorizes diagnoses based on severity and complexity, allowing payers to adjust reimbursements accordingly. HCC coding ensures that providers are properly compensated for treating high-risk patients.
How does HCC coding impact Medicare reimbursements?
Medicare uses HCC coding to determine reimbursement rates by assigning each patient a Risk Adjustment Factor (RAF) score based on their diagnoses. The higher the RAF score (indicating a sicker patient), the more Medicare will pay providers in a value-based care (VBC) model. Accurate HCC coding is crucial for ensuring fair and sufficient funding for patient care.
What is a risk adjustment factor (RAF) score in HCC coding?
A Risk Adjustment Factor (RAF) score is a numerical value assigned to patients based on their diagnoses, age, and demographics. Medicare and other payers use this score to estimate the cost of care for each patient. The higher the RAF score, the more financial resources are allocated for that patient’s healthcare needs.
How are ICD-10 codes mapped to HCC categories?
ICD-10 codes are mapped to HCC categories based on the severity and complexity of the diagnosed condition. Out of over 70,000 ICD-10 codes, approximately 9,500 are associated with one of the 86 HCC categories. Each ICD-10 code corresponds to a specific condition category in the HCC model, which reflects the patient’s risk of future healthcare costs.
Why should doctors outside of value-based care pay attention to HCC coding?
HCC coding isn’t just about reimbursement—it directly affects patient care. Accurate risk adjustment ensures that providers have a complete picture of a patient’s health, leading to better care coordination, appropriate treatment plans, and improved outcomes. As more healthcare models adopt risk-based payment structures, properly documenting chronic conditions will help ensure that patients receive the right care and support, regardless of the payment model.