PACE leaders are watching the Version 28 (V28) transition closely, and with good reason. Across Medicare Advantage, the conversation has been loud, reactive, and often misleading: “V28 slashed our RAF.” In many organizations, that narrative has driven anxiety, defensive posturing, and an assumption that revenue erosion is unavoidable.
For PACE programs, that framing misses the point.
The more accurate, and operationally useful, truth is this: V28 does impact revenue, particularly through the removal of lower-value diagnoses and changes in risk weighting. That impact, however, is not uniform or automatic. The degree of financial disruption is largely determined by documentation patterns, clinical workflows, and audit discipline.
Where documentation lacks clarity, clinical intent, or evidentiary support, V28 exposes those weaknesses more quickly and more forcefully. Where documentation is deliberate, compliant, and defensible, the revenue impact is materially more contained, and, in many cases, predictable.
This distinction matters especially in PACE, where care is longitudinal, patient acuity is high, and diagnoses are not episodic artifacts but reflections of ongoing clinical reality. The same model change that destabilizes other populations can, in PACE, act as a forcing function, shifting attention away from low-value coding behaviors and toward documentation practices that accurately reflect the complexity of the population being served.
Understanding that context is essential before talking about mitigation strategies, compliance risk, or RAF preservation. Because PACE is not just entering V28 with different patients, it is entering V28 with a fundamentally different advantage.
PACE is different, and that’s the advantage
Unlike traditional MA populations, PACE participants tend to present with higher-acuity, clinically significant conditions: advanced cardiovascular disease, cancer histories, ESRD, or neurologic impairment. These diagnoses largely remain in the V28 risk model.
What is disappearing are the “low-yield, easy-to-capture” conditions that inflated RAF under prior models. Their removal creates a measurable revenue gap, but in PACE, the proportional impact is smaller because baseline RAF is higher and driven by serious disease burden.
In other words:
The revenue gap is real, but for PACE it is mitigable, not catastrophic.
Understanding RAF declines in PACE: A documentation perspective
The steepest RAF drops are rarely caused by CMS alone. They stem from documentation behaviors that V28 exposes more aggressively:
1. Carrying acute diagnoses forward
Acute inpatient conditions (e.g., acute stroke) copied into outpatient or follow-up notes without clear clinical relevance remain a top audit risk. In V28, this behavior is more likely to be flagged, and reversed.
2. “Resolved” vs. active confusion
If a condition is resolved, it must be documented as history, not blended into an active problem list. This is a frequent EDS and RADV failure point.
3. Template overuse
PACE clinicians see patients frequently. When notes repeat verbatim while diagnoses change, or vice versa, documentation credibility erodes quickly.
These issues don’t just threaten RAF. They undermine audit defensibility, which is where financial risk compounds.
V28 raises the bar on clinical intent
What V28 really changes is where effort must be applied.
Success now depends less on finding every possible diagnosis and more on:
-
- Ensuring conditions are real, active, and supported
- Demonstrating clinical reasoning for complex, high-value diagnoses
- Aligning workflows to surface conditions that require evidence (e.g., imaging for Stage B heart failure)
For PACE programs, especially home-based models, this may require new logistics: transport to imaging, tighter screening protocols, and clearer physician education.
The compliance blind spot: documentation vs. submission
Many leaders conflate documentation loss with submission loss. They are not the same.
Documentation is what the clinician writes. Submission is how that data flows, through coders, vendors, and payers, to CMS.
While submission errors still occur, most V28 exposure originates in the note itself. That’s why relying solely on retrospective chart review is no longer sufficient.
This is where automation becomes leverage.
Operationalizing audit-ready documentation in PACE
High-performing PACE organizations are shifting from episodic audits to continuous documentation intelligence:
-
- AI-driven note review that evaluates 100% of encounters for MEAT, internal standards, and audit risk, before submission
-
- Point-of-care diagnosis guidance that helps clinicians focus on conditions that still matter under V28
-
- Targeted, clinician-friendly education delivered in short, repeatable formats that actually change behavior
This is how documentation becomes defensible by default, not corrected after the fact.
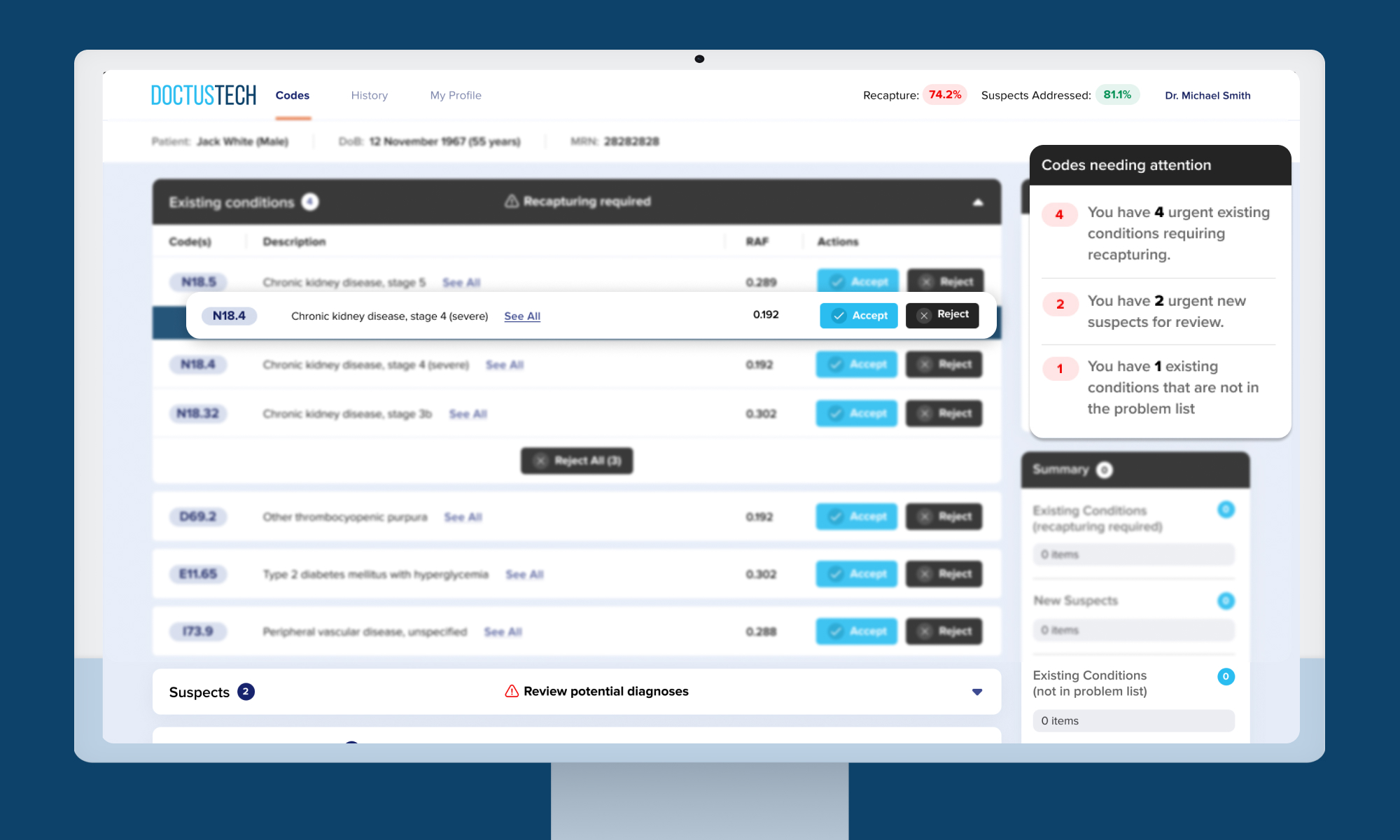
At DoctusTech, these principles are operationalized through:
-
- An AI Coder that scans every progress note for compliance and evidence alignment.
- A Diagnosis Assist platform that integrates directly into major EMRs to guide accurate HCC capture
- A Mobile Learning App that delivers individualized, weekly education to clinicians, supporting sustainable change without burnout
Not as add-ons, but as infrastructure.
So, when does PACE enter V28?
As of now, CMS has not finalized the exact implementation date for V28 within PACE programs. Industry guidance suggests alignment with upcoming payment years, anticipated in CY 2026, but PACE-specific timing has not yet been formally published by CMS.
That uncertainty makes one thing clear: waiting for a date is a losing strategy.
The bottom line for PACE leaders
V28 is not a documentation apocalypse for PACE. It is a stress test.
Organizations that:
-
- Understand their true diagnosis mix
- Eliminate risky documentation habits
- Invest in real-time compliance infrastructure
will stabilize their RAF and defend it confidently.
Those that don’t will continue blaming the model while bleeding revenue in audits.
The difference isn’t V28. It’s how prepared your documentation culture is to withstand it.
Ready to protect your organization? Get a Free Demo of DoctusTech’s solutions today.